By: Zoe Rosner
After 12 weeks of eating, sleeping and breathing clinical dietetics, I am happy to announce I still love it. Prior to beginning the program, I anticipated that clinical would be my favorite rotation and I was excited, though slightly anxious, to see if the experience would live up to my expectations. My first rotation placement for the internship was at Meritus Medical Center in Hagerstown, Maryland. I am happy to report that my major clinical rotation provided all I wanted and more.
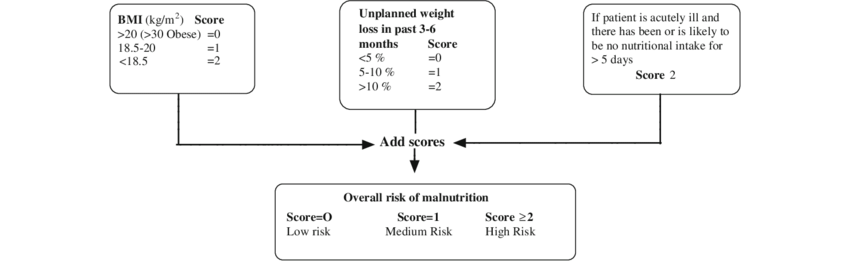
The diverse disease state knowledge and interdisciplinary experiences obtained during this rotation was invaluable. While I have known clinical to be a passion of mine because of previous work experience, I was lacking a breadth of knowledge in clinical dietetics. Working with a variety of dietitians with varying backgrounds and differing years of experience was a key component to my growth. Let me begin with the process of prioritizing patients, which was new and interesting to me. I had little knowledge regarding which patients needed to be seen and when, but after my first week it all made sense. Patients are screened at admission and will be seen by a dietitian if they report weight loss, decreased appetite or if they have a large wound prior to admission (see image for an example of a screening tool). Additionally, a dietitian reviews patient charts for all patients who stay in the hospital for more than five days and, if they are at nutritional risk the dietitian visits the patient. A patient may not be at risk upon admission, but during their stay they may lose weight or have poor intake, thus causing a dietitian to visit them. Lastly, a patient can be seen if another provider places a consult for the dietitian to see the patient. I learned to consider all the ways patients at nutritional risk are identified when organizing my day.
Kvamme J-M, Grønli O, Florholmen J, Jacobsen B. Risk of malnutrition is associated with mental health symptoms in community living elderly men and women: The Tromsø Study. BMC Psychiatry. 2011;11:112. doi:10.1186/1471-244X-11-112
Once patient load for the day is determined, next comes visiting with patients. Common patients at Meritus included those with disease states such as renal, cardiac, oncology, gastrointestinal, labor and delivery, rehabilitation and COVID-19. These individuals often included a mix of disease states, increasing the complexity. I recall during my fifth week of clinical practice, numerous patients were found to have bowel obstructions and were unable to eat anything by mouth to allow for gut rest. I was interested in following the day-to-day changes of these patients because their ability to consume nutrients would depend upon their medical status. Once an obstruction was resolved an oral diet could commence, but prior most patients were allowed only clear liquids, if that. Looking back, I believe I found these patients interesting because they posed a problem for me to solve. For instance, how could I provide adequate calories and protein to an individual consuming only clear liquids? Or what could I recommend to improve a patient’s nutrient intake so they wouldn’t need to be started on total parenteral nutrition? Being innovative and completing calculations is my favorite aspect of dietetics, so I was pleased I got to work many of these types of patients.
My interest in gastrointestinal diseases led me to return to one dietitian’s floors for my staff relief at Meritus. During staff relief I determined yet another patient population that sparked my interest. The floors I covered allowed me to see my fair share of bowel obstruction patients, a few recovering from bariatric surgery or COVID-19, and a variety of individuals taking part in inpatient rehabilitation. While I thought I was sold on GI, the inpatient rehab patients were also very interesting to me. Communicating with and working to improve oral intake for a patient actively recovering from a fall or stroke was an eye opening experience. A main concern with inpatient dietetics is providing immediate nutritional support to ensure a patients’ condition does not worsen. My inpatient rehab preceptor reminded me that good nutrition is key for patients’ recovery as they receive physical, occupational and speech therapy. Providing patients with enough energy to complete hours of therapy per day is essential and I found excitement in my role in doing so. Throughout staff relief I had a wonderful variety of patient types, which gave me a chance to think critically and use what I had learned during the time I spent at Meritus.

After watching a modified barium swallow with a speech language pathologist.
The best part about being a dietetic intern thus far has been the variety of experiences I have had right from the start with my first rotation. Working with dietitians who are excited to introduce new dietitians to the workforce, allowed me to learn from and connect with providers already in the field. I am excited to one day provide patient care just as they do. I cannot wait to jump back into clinical dietetics, but this time as a registered dietitian.